
Houston, The CDC Has a Problem (Part 2 of 3)
Four key insights reveal a CDC agenda of obfuscation and deception regarding SADS, cancer, and excess non-Covid mortality, along with attempts to make mRNA vaccines appear as effective as possible

As we survey the sizeable array of loose-end and speciously categorized data, it becomes readily apparent that the CDC is exhibiting all the symptoms of an organization which is constrained under the burden of a set of Kuhn-paradigm walking dead theories regarding Covid mortality.
Official data compromised so as to portray disinformation, is the warning sign that an entity, ostensibly one granted a government-authorized monopoly, under joint action to serve the American Public, is no longer serving science nor their fellow citizen – rather only social doctrines and out-of-control politics.

American philosopher Thomas Kuhn is credited with the proposition that science does not evolve gradually towards truth, but rather tends to anchor itself to a paradigm – a construct, notion, or hypothesis which bears the risk of remaining in play long past its shelf life. A theory thus can metastasize into a type of cult, zombie, or walking dead notion, if you will. Kuhn proposed that science therefore advances by what he called a paradigm shift and not merely by gradualism, nor especially through accretion of a set of conforming and convoluted explanatory gimmicks.
Such paradigm shifts occur in the particular circumstance where a current theory cannot sufficiently explain a phenomenon, and a coherent set of counter-observations have begun to accrue. A scientific revolution occurs when: (i) a new construct can be inferred directly from a set of these counter-observations; (ii) this novel paradigm offers superior explanatory power regarding the objective, observed reality; and (iii) the new paradigm runs heterogeneous to established (zombie) theory or narrative.1
A zombie theory is often times one which is sponsored and enforced by a syndicate. It will tend to be flagged for proactive support by its philosophical sycophancy, associated social movement, or allied political party. Such activity of course lends no credence whatsoever to the theory’s actual scientific validity.
When protection of a syndicate-sponsored idea becomes more important than the integrity of science itself, this is a particular form of zombie theory which ethical skepticism calls an Omega Hypothesis.
Within a previous article, we identified a mode and form of inference which we coined as heteroduction.2 Heteroduction is the very process of scientific inference which undertakes step (i) of the scientific revolution cycle identified by Kuhn. Heteroduction becomes of paramount importance in the presence of an enforced Omega Hypothesis.
A corporation or a political movement can become so fixated upon an established zombie theory, that its prevailing elements can rule as a form of pluralistic ignorance inside corporate ranks for years or decades – especially inside entities which do not operate in a market, and lack public scrutiny or competition. The entity or corporation will adopt a form of willful blindness toward its own foibles and fraud in support of its Omega Hypothesis. It will fail to self-check, begin to undertake borderline or even fully unethical activity in order to control what is known, and finally seek to actively suppress any form of dissent inside its ranks.
What the reader will observe below are a series of observations, a heteroduction if you will, signaling the presence of several Omega Hypotheses at play inside the US Centers for Disease Control and Prevention (CDC) – specifically the notion that Covid-19 has itself served as the sole origin of all the observed excess mortality in the US, and that we now face merely the aftermath of Covid-19’s wake, in the form of a pseudo-theory called ‘Long Covid’. A pseudo-theory is a mere notion enforced as science, which explains anything, everything, and nothing, all at the same time. Both of these notions have been falsified in spades. As we begin to examine and pull on the large set of tattered loose threads in the form of the database anomalies exhibited below, it becomes apparent that the CDC is exhibiting all the symptoms of an organization which is operating under the burden of a Kuhn-paradigm walking dead theory; and moreover, a politically-fueled Omega Hypothesis.
CDC MMWR Reporting Problem-Indicator Flags
The principal concerns with regard to the US Centers for Disease Control and Prevention Weekly Provisional Counts of Deaths by State and Select Causes and Wonder: Provisional Mortality Statistics are that the reports have begun to exhibit two primary apparent goals on the part of the CDC and its agency:
concealing excess deaths potentially caused by the mRNA vaccines, and
attempting to make mRNA vaccines falsely appear as uber-effective in saving lives.
Please note that we will not resolve an answer to either of these issues in this article, rather herein we will only outline the efforts in disinformation, misinformation, and deception on the part of the CDC which are foisted in an attempt to achieve both goals.
Accordingly, four key issues are entailed inside this two-sided-coin deception:
The National Vital Statistics System Upgrade (hereinafter referred to as the ‘NVSS System Upgrade’) afforded the CDC a timeframe inside which it could alter 22 weeks of NCHS-MMWR data. During this window of opportunity the CDC surreptitiously removed excess death records from its database, and adjusted the policies and techniques as to how ICD-10 mortality codes were populated with state death certificate data thereafter.
We outline herein that a new policy was enacted during the NVSS System Upgrade break, one which centered around two categorical gaming practices. The CDC is employing categorical gaming techniques to conceal dramatic Excess Non-Covid Natural Cause Mortality. If these excess deaths are not Covid deaths and are not vaccine related, as is commonly claimed through appeals to authority, credential, and ignorance, then there should also be no reason to conceal their associated records. Yet, that is exactly what is occurring.
Excess Cancer Mortality is being concealed through Cancer Multiple Cause of Death (hereinafter referred to as ‘MCoD’) categorical reassignment to Covid-19 Underlying Cause of Death (hereinafter referred to as ‘UCoD’).
Sudden Adult Deaths are being concealed by holding Pericarditis-Myocarditis-Conductive heart related deaths inside the R00-R99 temporary disposition bucket, far longer than per historical practice, thereby falsely depleting the associated ICD-10 mortality trend for these related deaths.
Finally, the CDC is using the exact opposite technique, exploiting Multiple Cause of Death attributions and adding in completely fictitious deaths as well, in order to make its mRNA vaccines appear to be performing better than they are.
The CDC is using Multiple Cause of Death categorical gaming, and is creating novel death counts, in order to counterfeit an appearance that the unvaccinated are dying at a rate twelve times that of the vaccinated.
These four issues are detailed as follows.
1. The NVSS System Upgrade Provided an Opportunity to Short and Reassign Death Records
The upgrade of the National Vital Statistics System (hereinafter, NVSS System Upgrade) was Machiavellian in its timing and opportunistic focus. In fact, as of October 2022 the entire evolution appears to have been a charade, crafted merely to obfuscate the set of warning indicators and activities outlined in this article. The NVSS System Upgrade provided an opportunity for the CDC to develop mechanisms to conceal Sudden Adult Deaths and Cancer Deaths (see Exhibit 1B below), and ironically only served to degrade the externally observable overall function and performance of the NCHS/State to CDC reporting process. Ostensibly, the process of final ICD-10 state death certificate record classification was to become tighter as a result of this upgrade. In the end, such benefit failed to manifest, as only Cancer Mortality reporting classification-lag actually appeared to improve. Yet even this ‘improvement’ in lag time turned out to be nothing more than the result of the CDC working to quickly hide cancer deaths in the first place (as documented in Exhibits 2A through 2D below). Overall, the NVSS System Upgrade was a failure – and only served to provide cover for surreptitious activity on someone’s part.3

The NVSS System Upgrade was slated to last 2 MMWR reporting weeks, yet ended up lasting a full 5 weeks longer than planned – thereby returning to its market with a full slate of shorted death records inside two specifically targeted ICD-10 code mortality sets, per Exhibit 1B below.
{kind=link}
{kind=link}
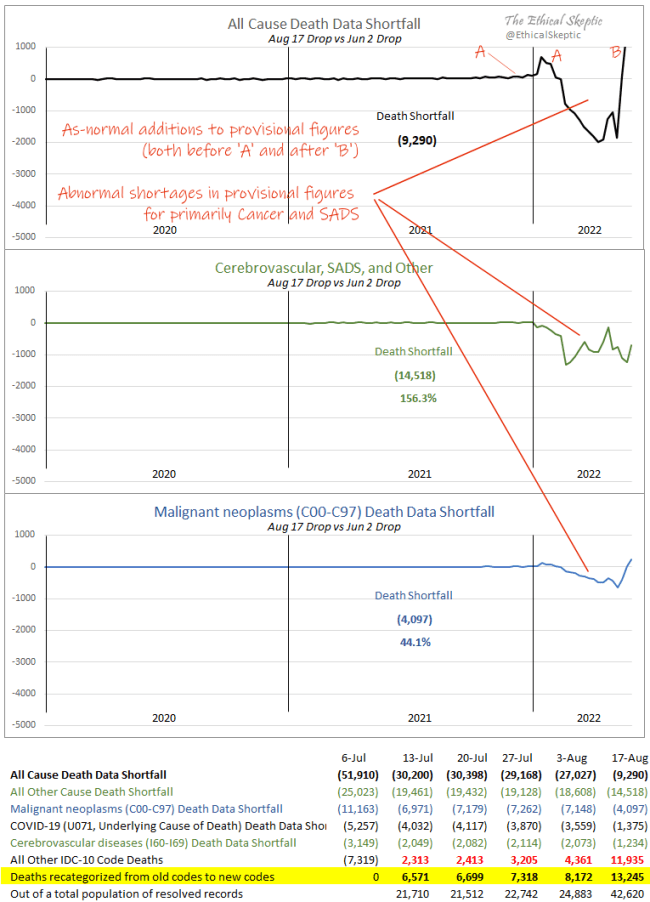
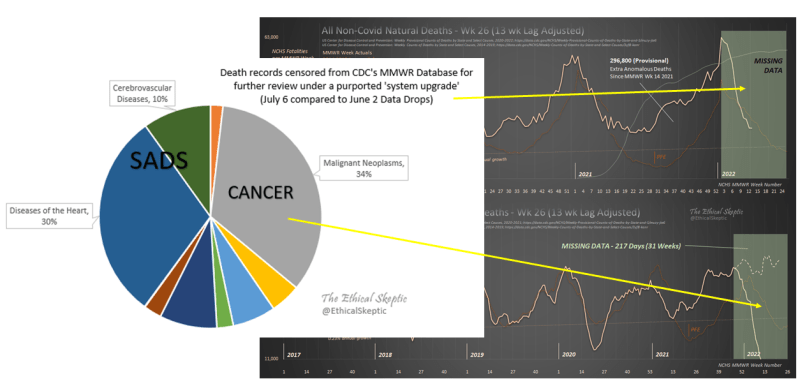
As of the last tally we conducted regarding records lost during the System Upgrade, of the 51,910 records which disappeared from the data during the seven week hiatus, 13,245 were reassigned to other ICD-10 death codes, while 9,290 records remained missing from the database altogether. 70% of these missing and reassigned records involved death certificates pertaining to Sudden Adult Deaths and Cancer Deaths. This was not accidental in the least. Those two ridiculously negative-impacted ICD-10 death charts are shown in Exhibit 1C below. Although they are silenced now by the successive weeks confirming that we were correct in our assessment, there were Narrative-driven persons who reviewed my material and insisted that I use these figures as fact in my analyses (falsely touting such condemnation as 'peer review'). I refused on the basis that I will not succumb to publishing Narrative disinformation.
Once this period cleared, and successive MMWR weeks were entered into the database, it became readily apparent that these sudden dips in mortality during the System Upgrade (the two right hand charts in Exhibit 1C above), were either erroneous or fraudulent in nature. Exhibits 2D and 6 show the corrected charts, as we continue below.
2. Categorical Concealment of Multiple Cause of Death Cancer Mortality
The NVSS System Upgrade afforded the CDC opportunity to both manipulate and excuse its reporting of cancer mortality, in order to obfuscate the 9-sigma excess in this ICD-10 code (C00-C97), a trend which had manifested early in 2022. The first signs of this obfuscation effort manifested immediately after the close of the System Upgrade, through a compression observable in the Cancer mortality death lag curve, per Exhibit 2A below. At first we attributed this lag curve compression to an actual improvement in record service time-to-data, as the CDC had indicated was the entire purpose of the NVSS System Upgrade.

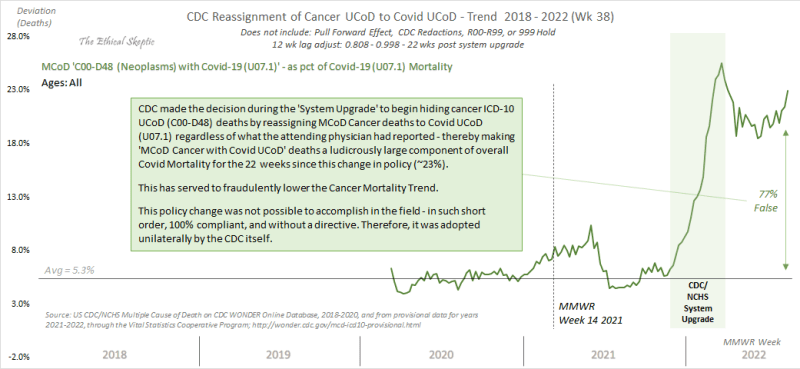
As it turned out, this ‘service time improvement’ presented as nothing more than a ruse. The cancer mortality lag curve compression which had been observed in Exhibit 2A above was merely an artifact of records being removed from the ICD-10 tally for cancer UCoD, occurring from week 2 through 18 of the provisional death lag period. In other words, the reason cancer deaths were hitting their long-term figure levels as soon as week -4 (all other ICD codes took 12 weeks to accomplish this), was because cancer deaths were being reassigned to Covid-19 UCoD deaths (see Exhibit 2D), or were being removed from the data altogether (see Exhibit 2E) after week -2 (per Exhibits 2B though 2E below). No wonder the lag cleared so fast.

In order to test just how ludicrous this reassignment of Multiple Cause of Death data is, in Exhibit 2C below one may observe that this quotient of cancer death reassignment to Covid-19 UCoD was not well thought out by the CDC at all. They left a loose end, an Irish Pennant, hanging about – and we caught it.
Since the NVSS System Upgrade, a full 25% of all Covid-19 mortality each week has just happened to be people also dying of cancer. Such constitutes an impossibility in this important mortality account ledger, one which is analogous to the same species of mistake an embezzler might make.†
(† Please note that I have had more than my share of embezzlers caught and intelligence cases broken during my career. I am well qualified in this professional activity.)
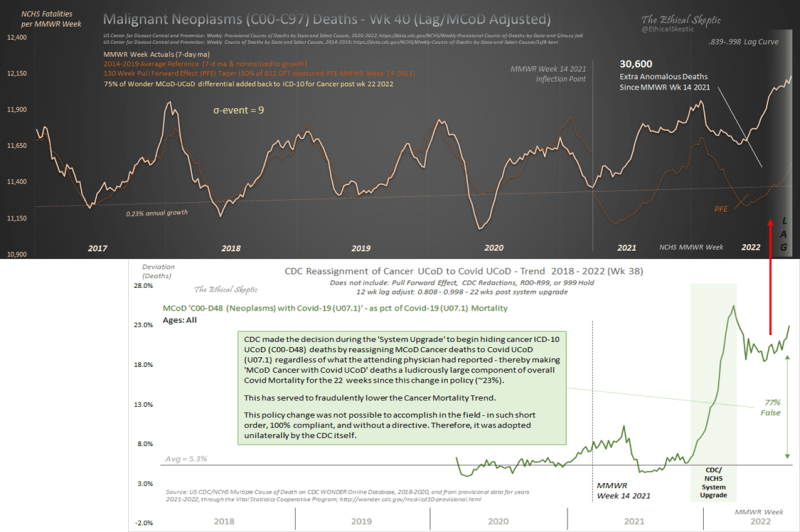
The net effect of this nefarious activity has been a shorting of 350 to 450 Cancer Underlying Cause of Death records from the ICD-10 database each week since the NVSS System Upgrade. When those death records are added back into the data (as they were prior to the System Upgrade) the Cancer Mortality trend resumes its 9-sigma cancer death excess which was observed immediately prior to the System Upgrade, and the cancer provisional lag comes back into alignment with the lag observed inside all the other ICD-10 codes, quod erat demonstrandum.
Finally, as one can see below, not satisfied with a mere re-assignment of cancer deaths over to Covid-19 death tallies, the CDC took this one step further and simply removed another 40 to 75 cancer death records from the MMWR database altogether, each and every week of the last 18 weeks. This broaches the question, is such a record reduction then normal? The answer to this question is an unequivocal ‘no’. Almost 100% of the provisional death records end up rising, not dropping, during the lag and provisional reporting period. This drop in cancer deaths is indicative of an exception activity at play on the part of those managing the MMWR reporting databases (Wonder data in the case cited in Exhibit 2E below). By itself, this might not mean that much. However, in light of the full set of nefarious activity centered on obfuscating both SADS and Cancer mortality, this exception too is indicative of fraud underway.

One can confirm these desperate attempts to obfuscate Cancer Mortality data by observing the ICD sub-sub code for Ill-defined and Secondary Site (C76-C80) cancers as well. This is an ICD-10 sub-sub code which normally makes up around 15% of all Cancer deaths each week. Post MMWR Week 14 2021 this sub-sub code suddenly composes 42% of all novel Excess Cancer Mortality. One can observe, by accessing this Cancer (C76-C80) meta-chart, that the CDC is particularly concerned about obfuscating the data for this category of entropy-indicating Cancer Mortality.
{kind=link}
One can also confirm such false Covid-19 UCoD attributions, by observing the stark but false rise in case fatality rates in the US in late 2022, as is depicted in this US Case Fatality Rate chart. Comparatively, the same chart for Europe features no such rise in CFR (converging around half the CFR of H1N1 flu, in line with most human coronavirus CFRs). Of course therefore, the World does not exhibit this CFR rise either. Only the US is stoking fear and hiding panic mistakes by means of false death accounting.
{kind=link}
{kind=link}
3. Categorical Concealment of Sudden Adult Death (Pericarditis/Myocarditis/Conductive Cardiac) Mortality
A paradox exists with regard to sudden young person and adult cardiac or anomalous deaths observable since mid 2021. Tens of thousands of cases of young persons dying suddenly in their sleep, or after a sporting event, are belied by a purported reduction in sudden cardiac death claimed by the CDC and pharmaceutical industry trolls, since the NVSS System Upgrade (see Exhibit 3B top panel).
One of my kids’ group of friends, a healthy young man who just finished college and was filled with hopes and dreams, suddenly died in his sleep of conductive heart failure several months ago. No drugs or alcohol were involved.
We were asked to believe (and it is only a belief), that these deaths ‘happen all the time’ and we were just not paying attention to them before. Bullshit – this is the same type of farce which was played upon us as parents of a child newly diagnosed with permanent disability encephalitis from vaccine injury years ago. I recognize the shtick. This is gaslighting.
In fact, those who enforce such pseudo-theory (remember, a theory which explains everything, anything, and nothing, all at the same time) hold absolutely no data to support their narrative dogma. It is maliciousness, pretending to be helpful. Below, we demonstrate why such activity constitutes gaslighting.
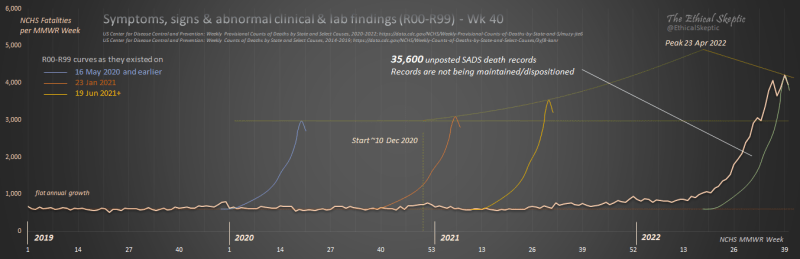
In Exhibit 3A below, one can observe that a temporary bucket exists which holds abnormal clinical and lab finding deaths (heavily represented by myocarditis, pericarditis, and conductive heart disorder deaths – because these are the deaths which most often serve to baffle doctors and coroners – as was the case with our family friend). Such deaths are not to be conflated with fentanyl or drug abuse deaths – which are easily detected through blood testing and are accounted for separately.
{kind=link}
During the period prior to MMWR Week 14 2021, to include the pandemic period, these deaths were resolved 90% to their final ICD-10 disposition across about 3 to 12 weeks. As one may observe in Exhibit 3A below, not only has this bucket of deaths grown by 70% since the introduction of mRNA vaccines into the US population, but as well, the CDC has decided to cease resolving these deaths to their final ICD-10 disposition. This has resulted in an estimated 35,600 abnormal clinical and lab finding pericarditis, myocarditis, and conductive disorder deaths which are not being accounted for in US Cardiac Mortality – thereby artificially depressing those ICD-10 mortality trend curves and allaying the conscience-nightmares of the pharmaceutical executive board members of the CDC.
This too, is no different than embezzlement of expense money or tax fraud inside a corporation or charity accounting ledger. Jim and Tammy Faye Baker would be impressed.
If one assigns a mere 18% of these anomalous and heavily cardiac deaths in younger persons, back to the Wonder data concerning myocarditis, pericarditis, and conductive heart disorder deaths – one gets a 22-sigma increase in this mortality sub-group since MMWR Week 14 of 2021. This process is shown in Exhibit 3B, and the result is indicated in its lower panel. In fact a very stark inflection in this data develops immediately commensurate with the roll-out of mRNA vaccines nationwide in the US.
My fear is that far more than 18% of these bucket-hold and unresolved deaths, involve abnormal and clinical findings related to pericarditis, myocarditis and conductive heart disorders – and the CDC is concealing a tsunami of a problem. This is a human rights crime.

In fact, if we prosecute this very inference which we inductively derived above, and test this deductively by querying the Wonder MCoD data for all Cardiac related deaths, including those RXX Abnormal & Clinical Lab Findings deaths which relate to abnormal heart-related conditions4 – those ostensibly held in the 22 week stasis cited above – one finds an alarming result. In the cases where there is no Covid-19 listed on the death certificate, we are at an all time high in heart-related deaths for the entire pandemic period. In fact a 17-sigma high (20-sigma with pull forward effect taken into account).
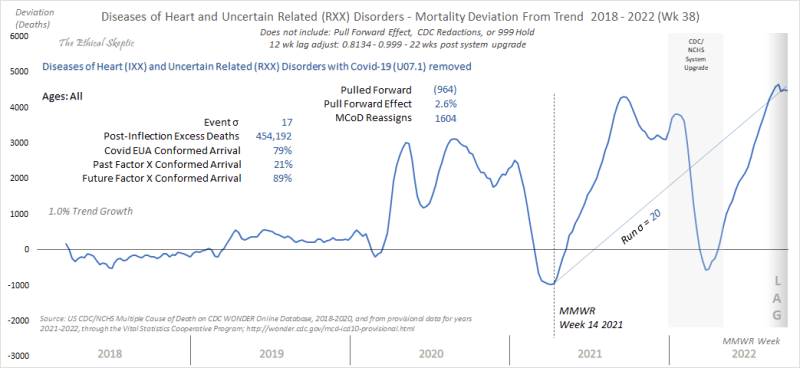
These excess Diseases of the Heart (IXX) and Uncertain Related Disorders (RXX) are not a result of Covid itself, despite the 2020 sympathy curves (Exhibit 3C 2020 blue line humps are in reality missed Covid and not a true increase in this ICD-10 code).5 This inflection and post-inflection signal should be lighting off warning alarms in all corridors of public health, … yet it is not. The combination of consilient inductive strength, reduced by convergent deduction – is tantamount to proof. Sorry pundits, your appeals to ignorance have only served to harm people.
4. Categorical Exploitation of Covid-19 MCoD Mortality to Coerce the Public with Case Fatality Rate Disinformation Regarding Vaccine Effectiveness
In Exhibit 4A below as well, one lays witness the accounting wherein suddenly, Multiple Cause of Death Covid-19 deaths are all assumed to be Underlying Cause of Deaths in solely the unvaccinated cohort. For the week analyzed in Exhibit 4A below, the Covid-19 MCoD tally for the week was 2,650 MCoD deaths (in the over-50 age bracket). Thus the CDC had to convert 841 MCoD deaths to UCoD deaths, and assign them only to the unvaccinated, and manufacture an additional 548 deaths more in that same cohort, in order to make the unvaccinated appear to have a 12 x case fatality rate as compared to the vaccinated cohorts. Rather than being executed inside a database however, this sleight of hand was accomplished in a sampling study instead – one where a reverse projection check was never done, in order to make sure that the results of the inductive projection study were sound – or in this instance, even possible.
These results are not mathematically possible.
This is coercion of innocent citizens by means of purposeful disinformation, and constitutes fraud.

Below in Exhibit 4B, we take the set exclusion calculations above in Exhibit 4A and portray them along the timeline of their arrival (23 weeks from 2 Apr to 3 Sep 2022), using the CDC’s very own analysis regarding death rates among 50+ year old vaccinated and unvaccinated cohorts.5 When these model calculations are extrapolated to the entire 50+ US population, suddenly a superfluous 12,656 death-count appears – conveniently in the timing and arrival form necessary to comprise the entire excess unvaccinated cohort death component. The superfluous deaths far exceed the 6,617 deaths necessary in fabricating the difference between the unvaccinated and vaccinated cohorts. The calculation base for Exhibit 4B below, which extends from the CDC model, can be seen by clicking here.
{kind=link}
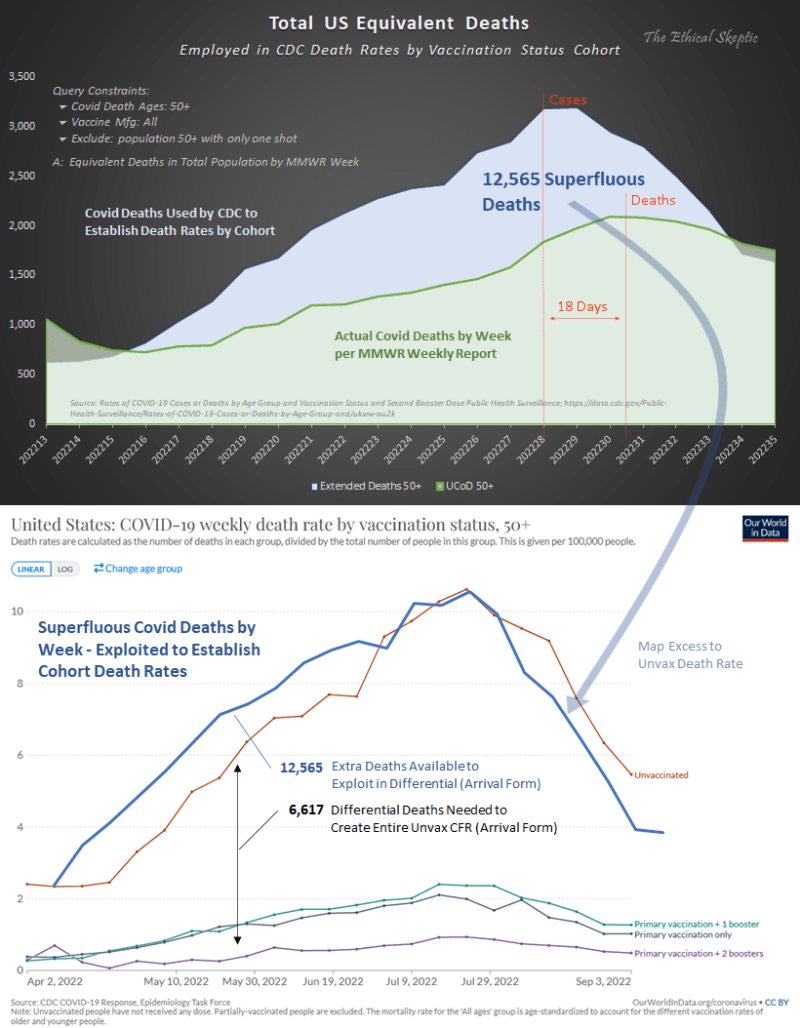
There is no doubt therefore, that the CDC and/or the surveillance hospital networks feeding this analysis, have manufactured superfluous deaths and inserted them in to the unvaccinated cohort death rolls, in order to fabricate a misleadingly high fatality rate among the unvaccinated as compared to the vaccinated. Inside this activity, the 18-day gap (shown in the upper panel of Exhibit 4B) between the vaccinated and unvaccinated cohort deaths is pivotal. The gap suggests that the following protocol was used to fabricate this cohort differential. Condition #1 below conforms with case arrivals and not the actual arrival of Covid deaths (18 days later).
Unvaccinated status + any UCoD + nosocomial Covid/no Covid = ‘Covid’ death
Vaccinated status + Covid + any MCoD = definitely not a Covid death (use the MCoD)
In other words, die of anything yet also be unvaccinated – then you ‘died’ of the suspected Covid you ‘caught’ upon entering hospital or hospice. Hence a peak sympathetic with cases, 18 days early. If vaccinated – then one could not possibly have had Covid, nor especially severe-Covid, therefore one didn’t die of Covid. A self-fulfilling model which functions upon the circular logic of constraints alone - one gets only that for which they constrain.
Moreover, the superfluous deaths quantified above in Exhibit 4B cannot be reconciled in any other fashion when constrained by the CDC model published above. The only place this magnitude of death differential can be accommodated in the CDC model, is by stuffing the superfluous death count for the period inside a skewed comparative – and the unvaccinated cohort death rate is the only one large enough to accommodate this large superfluous death count.
Thus, the unvaccinated death counts are falsely inflated and the cohort differentials are fraud, quod erat demonstrandum.
Addendum: The Yule-Simpson Effect Inside All Cause Mortality
Finally of course, it should be noted that the CDC attempts to define a pandemic and furthermore expresses its pandemic updates, in terms of All Cause Mortality. As epidemiological professionals in this case, they should not be using such a misleading metric. Pandemic risk at this juncture needs to be evaluated in terms of Excess Non-Covid Natural Cause Mortality (see Exhibit 6 below). This metric (the contrast of which can be observed in Exhibits 5 and 6) offers an indication of risk from Non-Covid death causes. As one can see in Exhibit 6 below, Excess Non-Covid Natural Cause Mortality is at an alarming 13.3% excess, while All Cause Mortality Excess (shown in Exhibit 5) stands at a rather nominal 3.3%. All Cause Mortality can therefore be deceptive when used as a stand-alone metric. Reader, be cautious of public health pundits who loosely spread unqualified All Cause Mortality figures.

In the end, it is this last chart depicted in Exhibit 6 which serves to confirm the claims made in Sections 1 through 4 of this article. The level of excess natural cause death which is not Covid itself, is around 13.3% to the excess of where it should be – even given a 1.1% baseline growth inside an aging demographic (see Exhibit 6, dark orange baseline ‘annual growth’).

While no other public health entity appears able to or interested in tracking this critical epidemiological metric, we not only track its anomalous magnitude, but we at The Ethical Skeptic believe we know what is causing these excess deaths as well. In fact, the data by ICD-10 sub-sub-code and by US County is starkly indicative, as well as condemning. No wonder the CDC is attempting to obfuscate it – as it will serve to infuriate those whom the CDC serves. Yes, organizations of this type operate under extreme levels of conflict of interest and agency. In the immortal words of Bob Dylan,
But you’re gonna have to serve somebody, yes
You’re gonna have to serve somebody
Well, it may be the devil or it may be the Lord
But you’re gonna have to serve somebody
We choose to stand in the gap for those who cannot defend themselves. Such unequivocal inference regarding the cause of these 385,000 excess natural cause deaths will be the subject of our third article in this series, ‘Houston, We Realize the Problem (Part 3 of 3)’. A problem which is rising at 7,340 deaths per week as of 8 October 2022 - and more importantly, does not appear to be abating any time soon.

The Ethical Skeptic, “Houston, The CDC Has a Problem (Part 2 of 3)”; The Ethical Skeptic, WordPress, 24 Oct 2022; Web, https://theethicalskeptic.com/?p=68500
It seems like they are always a few steps behind in the cover up if I am understanding things correctly. Then again most of them are Fed Gov employees. Which leads me to another point...
These Life long Fed employees would not be pulling this crap willingly for their meager salaries and threat of criminal retribution. So the dipshit Rachelle, Covid 1984 laid off all the employees except for an inner circle and pays them to stay home and do nothing which of course they enjoy. She hires with our money, her corrupt friends and family and some Eastern European math minds to fix the numbers. Wala they start changing the numbers.
Some new nefarious companies - Globalist agendas are trying to poison the pot further by combining the epidemiological areas moving forward I hear. What people will do for money. It is astounding. A new pair of shoes? 👠 a new car? 🚘 Doesn't it remind them every time they look at their prize how they lowered themselves to subhuman conscious-less levels to etch out a dog biscuit. Sorry, it is an insult to dogs. My dog seriously has more of a conscious.
What a bombshell piece, thank you so much for your work.